Regular readers of this blog, my magazine column, and my Twitter account, will know that I'm a passionate supporter of sepsis awareness.
As well as the tremendous work currently being undertaken by the UK Sepsis Trust to alert the public...and indeed, the medical profession...to its horrors and symptoms, the media also have a major part to play in getting the message across.
But it doesn't help anyone when the media sensationalise their stories by criticising doctors. Which is the point taken up by my guest blogger, today, Dr Alex Gates.
Dr Gates is a junior doctor, and member of the Royal College of General Practitioners AiT Committee. You can follow him on Twitter: https://twitter.com/dr_alex_gates
Here's what he has to say:
As well as the tremendous work currently being undertaken by the UK Sepsis Trust to alert the public...and indeed, the medical profession...to its horrors and symptoms, the media also have a major part to play in getting the message across.
But it doesn't help anyone when the media sensationalise their stories by criticising doctors. Which is the point taken up by my guest blogger, today, Dr Alex Gates.
Dr Gates is a junior doctor, and member of the Royal College of General Practitioners AiT Committee. You can follow him on Twitter: https://twitter.com/dr_alex_gates
Here's what he has to say:
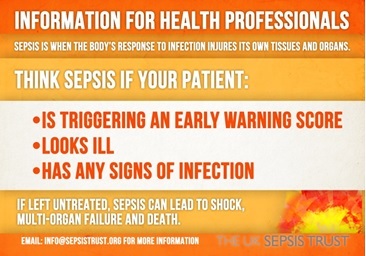
As a healthcare professional, there can arguably be no more important an issue than awareness of sepsis.
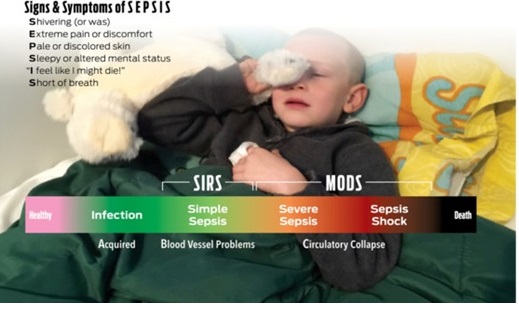
Sepsis, as the wider public are becoming increasingly aware, is deadly and gives little warning to the victim or their nearest and dearest. Perhaps the most common scenario the layperson will have encountered is the child or young adult with Meningococcal Septicaemia. For many years now there has been a drive to educate parents and students on the signs of meningitis and to encourage uptake of immunisation.
But what about awareness of sepsis in general? And how skilled are our junior doctors and GPs at spotting the often subtle signs of this rapid and severe disease process?
Sepsis, as the wider public are becoming increasingly aware, is deadly and gives little warning to the victim or their nearest and dearest. Perhaps the most common scenario the layperson will have encountered is the child or young adult with Meningococcal Septicaemia. For many years now there has been a drive to educate parents and students on the signs of meningitis and to encourage uptake of immunisation.
But what about awareness of sepsis in general? And how skilled are our junior doctors and GPs at spotting the often subtle signs of this rapid and severe disease process?
I don't wish to use this blog as an opportunity to simply defend the medical profession or exonerate those who have failed in their duty to protect a vulnerable patient. However, as a doctor it can be quite frustrating when there are numerous stories in the media portraying the whole profession as incompetent and negligent.
It would be remiss of me to discuss any individual tragic case that has been reported, and indeed some have garnered more media attention than others. A valid argument is that any publicity is good publicity, if it means people start to ‘think sepsis’. The common theme does, however, seem to involve ‘GP-bashing’ in individual cases where a patient (more commonly a child) has suffered harm or has even tragically died as a result of either individual or systemic failings.
It would be remiss of me to discuss any individual tragic case that has been reported, and indeed some have garnered more media attention than others. A valid argument is that any publicity is good publicity, if it means people start to ‘think sepsis’. The common theme does, however, seem to involve ‘GP-bashing’ in individual cases where a patient (more commonly a child) has suffered harm or has even tragically died as a result of either individual or systemic failings.
 | I was angered on the 8th October 2016 when I read a story by the Press Association entitled ‘GPs neglect four tests on young with fever which could flag up threats to life'. Click title to read article. The article, based on research presented at the Royal College of General Practitioners’ Annual Conference, packs a punch in its opening statement: ‘GPs are failing to carry out basic checks on children with fever that could flag up life-threatening illnesses, research suggests. |
'A new study found most under-fives with a high temperature are not checked properly for signs that could indicate sepsis, meningitis or pneumonia.’
What the reader subsequently discovers is that this was a small study of just 47 children consulting their GP with a fever in a single GP practice. This is of negligible statistical significance, so why this attracted the attention of the national media is not clear. The point is, of course, that it only takes ONE missed opportunity to misdiagnose a child. And early recognition of sepsis is essential, which is why it is so important these parameters are recorded.
The context is vitally important. The National Institute of Clinical Excellence (NICE) published clear guidance in 2013 that such children presenting with a febrile illness should have four parameters checked and recorded – Respiratory Rate, temperature, heart rate and capillary refill time. These are essential in differentiating a child with a self-limiting viral illness from one at risk of rapid deterioration. Whilst it is disappointing that the study found only 13% of consultations included all 4 checks, it would be a gross oversimplification to suggest the entire GP workforce is guilty of wilfull negligence!
What the reader subsequently discovers is that this was a small study of just 47 children consulting their GP with a fever in a single GP practice. This is of negligible statistical significance, so why this attracted the attention of the national media is not clear. The point is, of course, that it only takes ONE missed opportunity to misdiagnose a child. And early recognition of sepsis is essential, which is why it is so important these parameters are recorded.
The context is vitally important. The National Institute of Clinical Excellence (NICE) published clear guidance in 2013 that such children presenting with a febrile illness should have four parameters checked and recorded – Respiratory Rate, temperature, heart rate and capillary refill time. These are essential in differentiating a child with a self-limiting viral illness from one at risk of rapid deterioration. Whilst it is disappointing that the study found only 13% of consultations included all 4 checks, it would be a gross oversimplification to suggest the entire GP workforce is guilty of wilfull negligence!
An experienced GP will have a ‘trained eye’ for spotting the worryingly sick child. They will rely not just on numbers, but on the child’s medical history, the social situation and any parental concerns. This ‘instinct’ is not infallible, but neither should it be replaced by a set of data. A safe clinical assessment comprises evidence, instinct and so-called ‘safety-netting’.
That is, every time a GP reviews a patient they are only getting a small snapshot of their health and so must make a clear plan for what the patient should do in the event things get worse. The evidence you glean during those ten minutes is only representative of that small window and the transition and rapidity from a state of reasonable health to one of severe disease or danger to life can be very difficult to predict.
This makes our job incredibly hard, and as such we must always be confident that we are empowering patients to make sound decisions if clinical need changes. As such, every consultation with a poorly child will conclude with a robust plan for what the parents should do in the event the child deteriorates or they are worried. This is not to abscond ourselves of responsibility, but it is a realistic acknowledgement that children are very good at compensating right up until the point when an infection becomes overwhelming and their bodies enter a state of sepsis.
The signs of sepsis are often late too, for instance the classical ‘non-blanching’ rash of meningitis is a late, often terminal sign.
That is, every time a GP reviews a patient they are only getting a small snapshot of their health and so must make a clear plan for what the patient should do in the event things get worse. The evidence you glean during those ten minutes is only representative of that small window and the transition and rapidity from a state of reasonable health to one of severe disease or danger to life can be very difficult to predict.
This makes our job incredibly hard, and as such we must always be confident that we are empowering patients to make sound decisions if clinical need changes. As such, every consultation with a poorly child will conclude with a robust plan for what the parents should do in the event the child deteriorates or they are worried. This is not to abscond ourselves of responsibility, but it is a realistic acknowledgement that children are very good at compensating right up until the point when an infection becomes overwhelming and their bodies enter a state of sepsis.
The signs of sepsis are often late too, for instance the classical ‘non-blanching’ rash of meningitis is a late, often terminal sign.
| This is absolutely not about making excuses. A medical professional, Trust or care provider must absolutely be held to account in cases where there has been clear negligence or there is evidence that a full clinical assessment has not been carried out, or subsequent harm has occurred. But is it helpful to suggest that all GPs are liable to making the same mistakes? I really don’t think so. Blame is so easily and rapidly dealt in situations where a life has been tragically lost, and it is easy (and often justified) to hold individuals to account for their actions. | 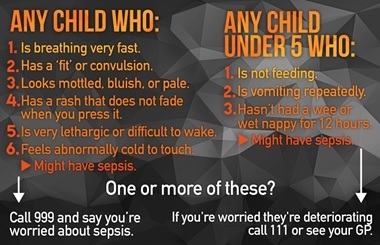 |
But what about the more understated system-wide failings which contribute to these (fortunately rare) tragedies? We must ask ourselves whether clinicians have adequate resources to practice safely. This, broadly speaking, is the debate which sparked the whole Junior Doctor dispute which has become so bitter and convoluted. Patients are coming to harm, on a daily and increasing basis, due to cutbacks, staff shortages and service closures. This harm is pretty difficult to quantify and equally difficult to hold the perpetrators – those responsible in government – to account. It frustrates me hugely that there seems to be a complete lack of accountability in the current political stratospheres.
You may ask, are doctors receiving enough training in sepsis and child health? I can testify that, during my undergraduate training and 5 years practicing as a doctor, sepsis is one of the most widely taught and discussed topics. It is drummed into us from the moment we hit the wards. Here, we have special proformas, numerous memoranda, training bundles and specially trained nurses to identify early those patients at risk from sepsis and intervene. The challenge is when patients are in the community, and there are no sepsis nurses, lab tests or regular observation charts to assist in diagnosis and risk stratification.
GPs are perhaps as vulnerable as their patients in this sense, and must work with what little equipment and information they have at their disposal. And, as we are only human, very occasionally errors do occur. This is where it becomes vital to ensure this risk is minimised through improved training and confidence in assessing children. Many current campaign resources are targeted at hospital doctors leaving those in Primary Care rather exposed. There are several excellently-designed online educational tools that doctors can use, but one thing I am keen to pursue is for every GP trainee to undertake a period of mandatory hospital-based paediatrics training to gain insight into what a sick child looks like and how they behave physiologically. Not all doctors in GP training have the opportunity to rotate through a Paediatrics job, unfortunately, meaning some may have very limited experience.
In order to foster a culture of competence and confidence in this area, we need to empower doctors and not chastise them. It can be harmful not just to the morale of the medical profession, but to the relationship and trust we build with patients, when headline-grabbing stories of harm, neglect and tragedy circulate. But ultimately the very worst harm is that suffered by the child and family. We must empower parents and patients, and we must ensure all thinking in the NHS is linear and ‘joined-up’. The moment the pieces of the jigsaw become dispersed the system can fail and human tragedy, unfortunately, is inevitable.
The NHS needs both adequate funding and confident, assured leadership to thrive and the ‘make-do’ and ‘efficiency saving’ culture we are increasingly seeing will ultimately be far more harmful to patient safety than the actions of one clinician. Let’s all work together to improve outcomes and awareness.
For more information about sepsis, take a look at The Sepsis Trust website: http://sepsistrust.org/
You may ask, are doctors receiving enough training in sepsis and child health? I can testify that, during my undergraduate training and 5 years practicing as a doctor, sepsis is one of the most widely taught and discussed topics. It is drummed into us from the moment we hit the wards. Here, we have special proformas, numerous memoranda, training bundles and specially trained nurses to identify early those patients at risk from sepsis and intervene. The challenge is when patients are in the community, and there are no sepsis nurses, lab tests or regular observation charts to assist in diagnosis and risk stratification.
GPs are perhaps as vulnerable as their patients in this sense, and must work with what little equipment and information they have at their disposal. And, as we are only human, very occasionally errors do occur. This is where it becomes vital to ensure this risk is minimised through improved training and confidence in assessing children. Many current campaign resources are targeted at hospital doctors leaving those in Primary Care rather exposed. There are several excellently-designed online educational tools that doctors can use, but one thing I am keen to pursue is for every GP trainee to undertake a period of mandatory hospital-based paediatrics training to gain insight into what a sick child looks like and how they behave physiologically. Not all doctors in GP training have the opportunity to rotate through a Paediatrics job, unfortunately, meaning some may have very limited experience.
In order to foster a culture of competence and confidence in this area, we need to empower doctors and not chastise them. It can be harmful not just to the morale of the medical profession, but to the relationship and trust we build with patients, when headline-grabbing stories of harm, neglect and tragedy circulate. But ultimately the very worst harm is that suffered by the child and family. We must empower parents and patients, and we must ensure all thinking in the NHS is linear and ‘joined-up’. The moment the pieces of the jigsaw become dispersed the system can fail and human tragedy, unfortunately, is inevitable.
The NHS needs both adequate funding and confident, assured leadership to thrive and the ‘make-do’ and ‘efficiency saving’ culture we are increasingly seeing will ultimately be far more harmful to patient safety than the actions of one clinician. Let’s all work together to improve outcomes and awareness.
For more information about sepsis, take a look at The Sepsis Trust website: http://sepsistrust.org/
 RSS Feed
RSS Feed
